Challenging ASD closure!
42 mm secundum ASD with persistent AF.
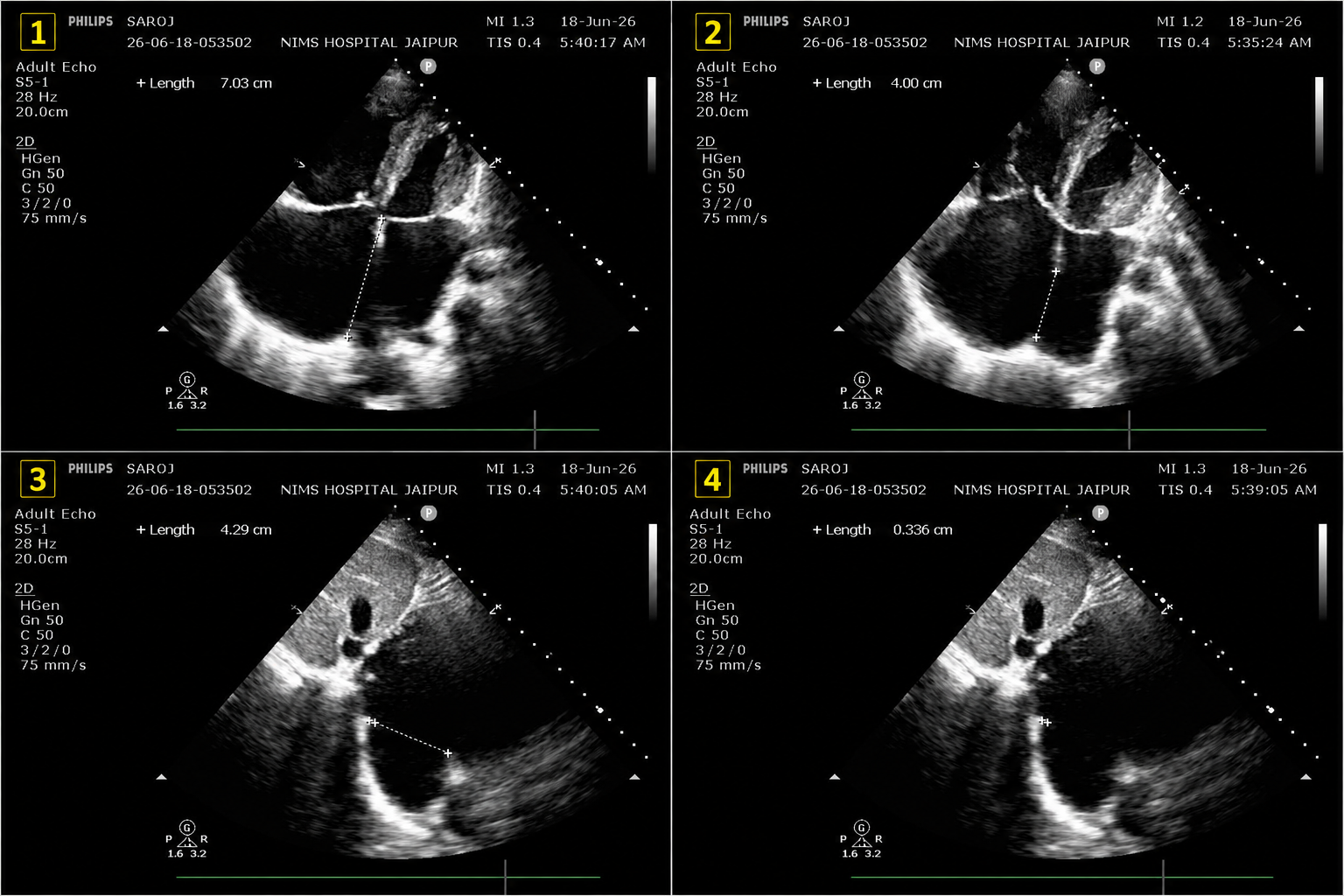
Rims
- IVC rim: 3 mm
- Posterior rim: 4–5 mm
- Aortic, SVC & mitral rims: adequate
- Septal length: 70 mm
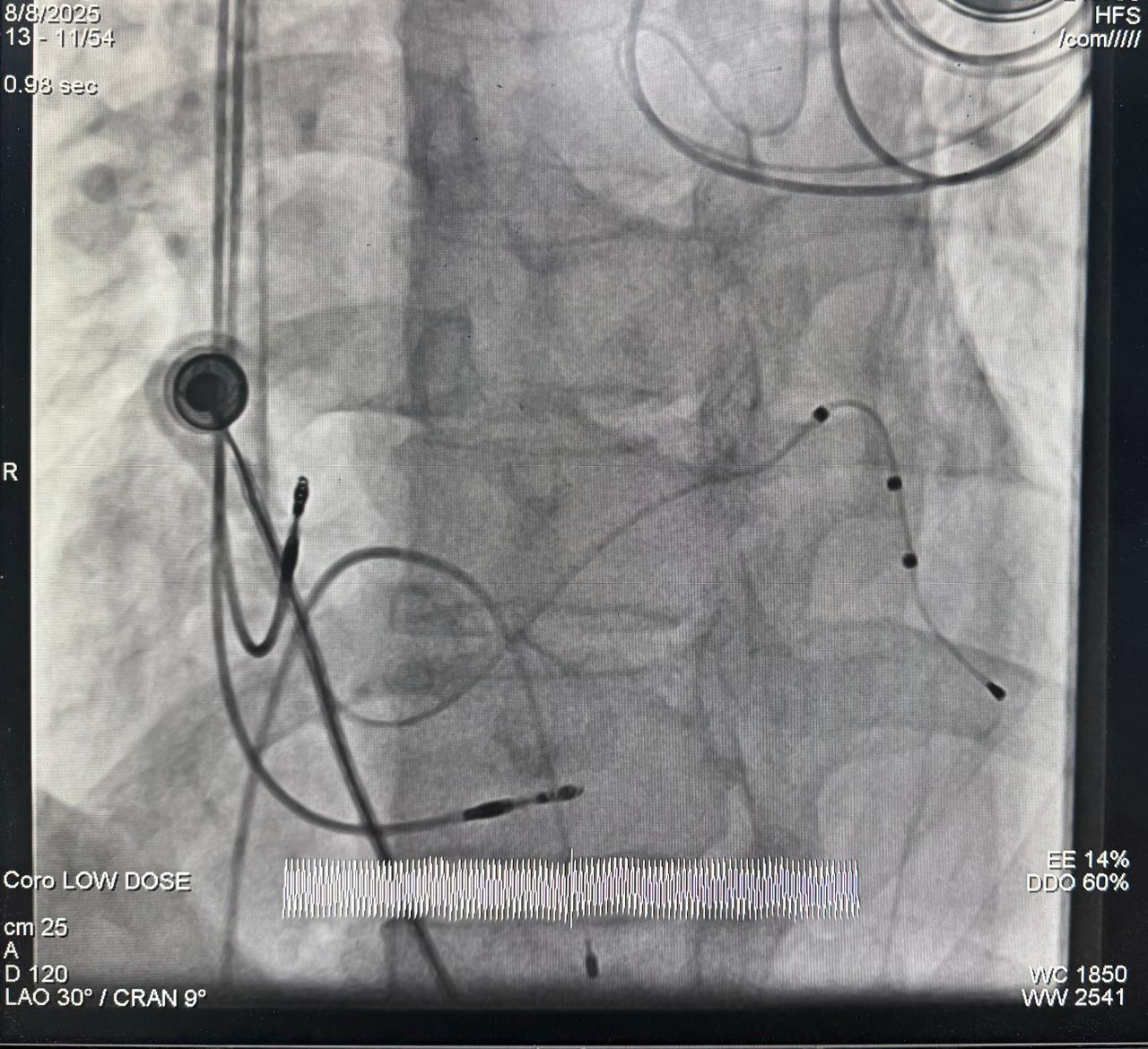
Initial deployment with both RUPV and LUPV techniques failed. Finally, successful implantation of a 48 mm ASD occluder using the LA roof technique under fluoroscopic + transthoracic echocardiographic (TTE) guidance.
Structural heart interventions continue to evolve, allowing increasingly complex atrial septal defects (ASDs) to be treated using minimally invasive techniques. This case highlights the successful closure of a large secundum ASD using a 48 mm ASD device under local anaesthesia with fluoroscopic and transthoracic echocardiographic guidance alone, without TEE.
Case Overview
The patient presented with a large 42 mm secundum ASD associated with persistent atrial fibrillation (AF). Detailed anatomical assessment revealed significant procedural challenges due to deficient septal rims.
Anatomical Findings
- ASD Size: 42 mm secundum ASD
- Persistent Atrial Fibrillation
- IVC Rim: 3 mm
- Posterior Rim: 4–5 mm
- Aortic Rim: Adequate
- SVC Rim: Adequate
- Mitral Rim: Adequate
- Septal Length: 70 mm
The severely deficient IVC rim and limited posterior rim made device positioning particularly challenging.
Procedural Challenges
Large ASDs with deficient rims are among the most demanding structural heart interventions. Initial deployment attempts using both the Right Upper Pulmonary Vein (RUPV) and Left Upper Pulmonary Vein (LUPV) techniques were unsuccessful.
Successful Deployment Using the LA Roof Technique
After conventional deployment strategies failed, the Left Atrial (LA) Roof Technique was utilized. This approach provided optimal alignment and stability, allowing successful implantation of a 48 mm ASD device despite the severely deficient IVC rim.
The procedure was completed successfully with excellent device positioning.
Clinical Significance
This case demonstrates that even very large ASDs with severely deficient rims can be successfully managed through transcatheter techniques when appropriate expertise and advanced deployment strategies are employed.
Conclusion
Careful anatomical assessment and mastery of advanced deployment techniques enable successful ASD closure even in highly complex anatomical situations. This case adds valuable experience to the field of structural heart interventions and supports feasibility of complex ASD closure under fluoroscopic and TTE guidance alone, without TEE.